

Standard schedule:
Administered as a 1-hour IV infusion every 3 weeks across multiple indications.1
Preparing Beizray1
-
Calculate
-
Beizray:Beizray (docetaxel) dose (mg/m2) x Body Surface
Area (m2) ÷ 20 mg/mL = Beizray (docetaxel) dose (mL)Select IV bag:Beizray ≤ 8.8 mL = 500 mL
Beizray > 8.8 mL = 1,000 mLAlbumin:Beizray (docetaxel) dose (mL) x 6 =
Albumin dose (mL) -
Albumin:
-
Add to IV bag, mix by gently inverting bag at least 5 times. Do not shake.
-
Beizray:
-
Add to IV bag, mix by gently inverting bag at least 10 times. Do not shake.
For complete preparation and administration instructions, please see the full
Prescribing Information , including Boxed WARNING.
Watch how Beizray is prepared
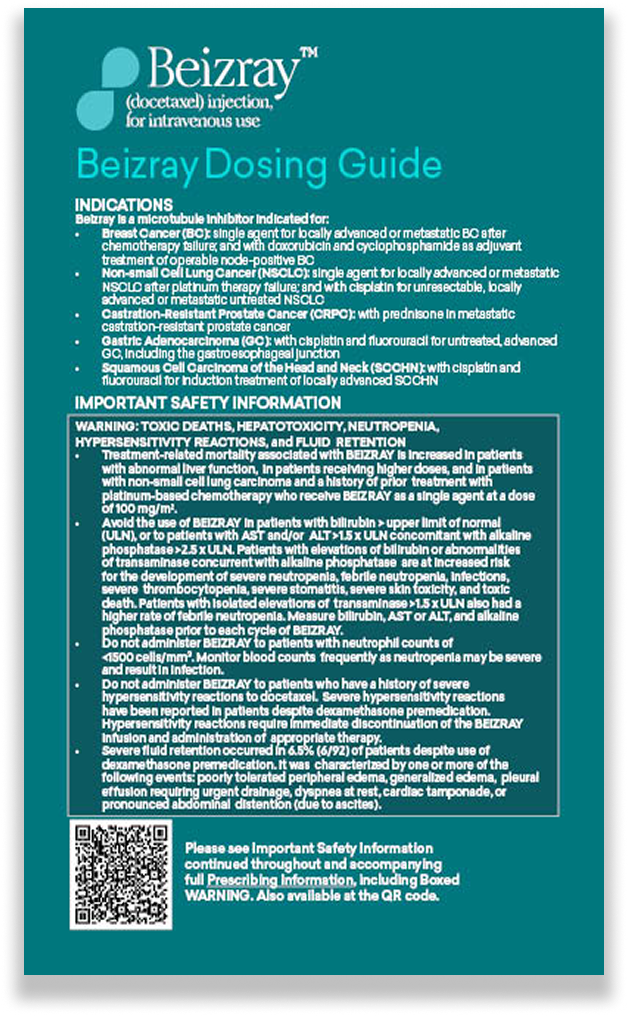
Beizray follows the same dosing as docetaxel across indicated tumor types
Weight-based (BSA) dosing:
Typical starting dose is 75 mg/m² across most indications.1
Premedication requirements:
Corticosteroid premedication is required to reduce the incidence and severity of fluid retention and hypersensitivity reactions. Please see Boxed WARNING and Warnings and Precautions in the full Prescribing Information.1
Clear modification rules:
For all indications, toxicities may warrant dosage adjustments. Beizray utilizes the same dose modifications as the reference drug, Taxotere®. See full Prescribing Information for details.1,9
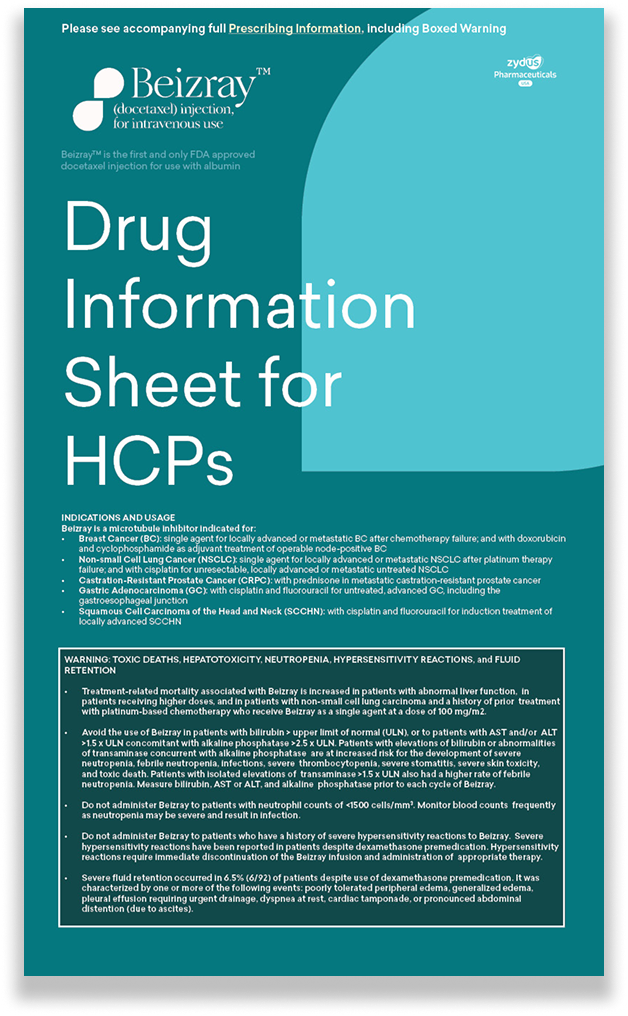
Important Dosage and Administration1 Instructions
- Do not substitute BEIZRAY for or with other docetaxel products because BEIZRAY has different administration instructions from other docetaxel products.
- For all indications, toxicities may warrant dosage adjustments.
- Administer in a facility equipped to manage possible complications (e.g., anaphylaxis).
- See additional premedication recommendations for the indicated populations.
J9174
All Beizray NDCs (National Drug Code) crosswalk to J9174

Recommended Dosage1









Corticosteroid Premedication Regimen1
All patients should be premedicated with oral corticosteroids (see below for prostrate cancer) such as dexamethasone 16 mg per day (e.g., 8 mg twice daily) for 3 days starting 1 day prior to BEIZRAY administration in order to reduce the incidence and severity of fluid retention as well as the severity of hypersensitivity reactions.
For metastatic castration-resistant prostate cancer, given the concurrent use of prednisone, the recommended premedication regimen is oral dexamethasone 8 mg at 12 hours, 3 hours, and 1 hour before the BEIZRAY infusion.
To report SUSPECTED ADVERSE REACTIONS, contact Zydus Pharmaceuticals (USA) Inc. at 1-877-993-8779 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see the full Prescribing Information, including BOXED WARNING
Beizray Calculation Examples
The following chart is for informational purposes only and is an example intended to guide preparation once a calculated dose has been obtained.10
Calculated dose should be based on the recommended dose by indication and body surface area of your patient per the Prescribing Information.
0 mg
- 0 mg
- 60 mg
- 65 mg
- 70 mg
- 75 mg
- 80 mg
- 85 mg
- 90 mg
- 95 mg
- 100 mg
- 105 mg
- 110 mg
- 115 mg
- 120 mg
- 125 mg
- 130 mg
- 135 mg
- 140 mg
- 145 mg
- 150 mg
- 155 mg
- 160 mg
- 165 mg
- 170 mg
- 175 mg
- 180 mg
- 185 mg
- 190 mg
Calculated Beizray Dose
(mg)
(mg)
25% Albumin
(mL)
(mL)
Calculated Beizray
Volume
(mL)
Volume
(mL)
Kits*Vials
160 mg (8 mL)
80 mg (4 mL)
20 mg (1 mL)
* Kits include Beizray + Albumin
Bag size (mL)
Total Vol. (mL)
ZySupport™
With You at Every Step

ZySupport™ offers a full suite of solutions to address common hurdles to access and reimbursement such as:
- Benefits verification for patient coverage and out-of-pocket responsibilities
- Payer-specific guidance for prior authorizations & appeals to address patient needs
- Solutions for insurance-related delays
ZySupport has resources to help your patients get started and stay on their prescribed Zydus medication.
Our reimbursement experts are available to help assist with coverage, prior authorization, appeals, co-pay support, and more to help patients start and stay on their prescribed Zydus medicines — regardless of insurance type.*
* Terms and conditions apply
For more information, or to speak with a Patient Access Specialist dial 866-891-9938
Hours: 8am-8pm ET, Monday-Friday
Download ZySupport leaflet (PDF)
Regional Beizray support
[Selected State]
Select State
State Representative
[State representative]
[email address]
Field Reimbursement Manager
[Field Reimbursement Manager]
[email address]
Beizray has National
Medicare MAC Coverage
Regional Beizray support
Zydus and its agents make no guarantee regarding reimbursement for any service or item. The accurate completion of reimbursement- or coverage-related documentation is the responsibility of the healthcare provider and patient. For eligibility requirements, please contact a patient assistance specialist.
To report adverse events or product complaints please email medicalaffairs@zydususa.com,
call 877-993-8779, or fax +1-609-559-0699 or contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
